A 50 year old female patient with ANASARCA AND DECREASED URINE OUTPUT
Medical case disscussion
 ●Ultrasound:
●Ultrasound:

11-2-22
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent
Here we discuss our patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs
This E log book also reflects my patient - centered online learning portfolio and your valuable inputs inthe comment box are welcome.
Name : Mounika 7th sem
Roll no : 46
I have been given this case to solve an attempt to understand the topic of "patient clinical analysis data " to develop my competency in reading and comprehending clinical data including clinical history,clinical findings, investigations and come up with a diagnosis and treatment plan
50 YO FEMALE WITH ANASARCA, DECREASED URINE OUTPUT AND SOB
50 year old female a resident of Suryapet got admitted to the hospital on 11/02/22 with the CHIEF COMPLAINTS of:
Generalized edema since 10 days
○HOPI:
The patient was complaining of pedal edema on and off since 2 months and generalized edema since 10 days which started from legs and then whole body swelling , which was not associated with pain and did not subside on taking medication.
Then 3 days later she started developing shortness of breath , which was progressive in nature initially she had SOB where she could not do even minimal activity ( Grade 3 NYHA ),There was no diurnal variation and then from past 5 days she is having SOB even while she was lying down(Grade 4NYHA)
No history of : Fever,Exertional Dyspnoea, Dysurea,Haematuria,Loss of appetite, Oliguria,Nausea, Vomitings, Diarrhoea, Burning micturation.
○PAST HISTORY:
She had similar complaints in the past.
Appetite: Normal
Sleep: Adequate
○FAMILY HISTORY:
Her father died after developing ANASARKA when he's 60 years old
○GENERAL EXAMINATION:
The patient was examined in a well lit room after obtaining consent.
The patient was conscious, coherent and cooperative. She was moderately built and moderately nourished.
Pallor: present
Icterus: Absent
Cyanosis: Absent
Clubbing: Absent
Lymphedenopathy: Absent
Edema: whole body




 Temperature: 98.6°F
Temperature: 98.6°F
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent
Here we discuss our patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs
This E log book also reflects my patient - centered online learning portfolio and your valuable inputs inthe comment box are welcome.
Name : Mounika 7th sem
Roll no : 46
I have been given this case to solve an attempt to understand the topic of "patient clinical analysis data " to develop my competency in reading and comprehending clinical data including clinical history,clinical findings, investigations and come up with a diagnosis and treatment plan
50 YO FEMALE WITH ANASARCA, DECREASED URINE OUTPUT AND SOB
50 year old female a resident of Suryapet got admitted to the hospital on 11/02/22 with the CHIEF COMPLAINTS of:
Generalized edema since 10 days
SOB since 1 week which progressed from grade 3 to grade 4
○HOPI:
The patient was complaining of pedal edema on and off since 2 months and generalized edema since 10 days which started from legs and then whole body swelling , which was not associated with pain and did not subside on taking medication.
Then 3 days later she started developing shortness of breath , which was progressive in nature initially she had SOB where she could not do even minimal activity ( Grade 3 NYHA ),There was no diurnal variation and then from past 5 days she is having SOB even while she was lying down(Grade 4NYHA)
No history of : Fever,Exertional Dyspnoea, Dysurea,Haematuria,Loss of appetite, Oliguria,Nausea, Vomitings, Diarrhoea, Burning micturation.
○PAST HISTORY:
She had similar complaints in the past.
1 year back she had pedal edema for which she went to hospital and was diagnosed with AKI
The patient is a known case of
The patient is a known case of
Diabetes for the past 15 years and was under medication
The patient was diagnosed with Diabetes when she went to a local hospital with complaint of dizziness.
The patient is also a known case of
Hypertension for the past 3 months and was under medication
The patient was diagnosed with HTN when she went to a local hospital with complaints of pedal edema and diminished vision.
No other comorbidities
Patient is not a known case of TB, Asthama,Epilepsy, Thyroid abnormalities
○PERSONAL HISTORY:
Diet: Mixed
The patient was diagnosed with HTN when she went to a local hospital with complaints of pedal edema and diminished vision.
No other comorbidities
Patient is not a known case of TB, Asthama,Epilepsy, Thyroid abnormalities
○PERSONAL HISTORY:
Diet: Mixed
But she's taking only vegetarian diet since a year
Appetite: Normal
Sleep: Adequate
But she's experiencing SOB since 5 days
Bowel: Regular
Bladder: Decreased urineation.
Habits: She consumed toddy (30ml)daily in the evening and alcohol occasionally since childhood (her father was a toddy person)
Bowel: Regular
Bladder: Decreased urineation.
Habits: She consumed toddy (30ml)daily in the evening and alcohol occasionally since childhood (her father was a toddy person)
But she stopped taking toddy and alcohol 1 year back when she was diagnosed with AKI
○FAMILY HISTORY:
Her father died after developing ANASARKA when he's 60 years old
He died because he was not treated
○DRUG HISTORY:
Some oral antidiabetic drug
TELMA for hypertension since the past 3 months.
○DAILY ROUTINE:
Until 3 years ago she worked as a daily wage labourer,and stopped working because she developed diminision of vision.
○DRUG HISTORY:
Some oral antidiabetic drug
TELMA for hypertension since the past 3 months.
○DAILY ROUTINE:
Until 3 years ago she worked as a daily wage labourer,and stopped working because she developed diminision of vision.
She wakes up at 6 am. She has her tea at 7 am. Then does some household work ,Then she has breakfast at 9 am . She then has lunch at 1 pm. Dinner at 7 pm and goes to bed at 9 pm.
○GENERAL EXAMINATION:
The patient was examined in a well lit room after obtaining consent.
The patient was conscious, coherent and cooperative. She was moderately built and moderately nourished.
Pallor: present
Icterus: Absent
Cyanosis: Absent
Clubbing: Absent
Lymphedenopathy: Absent
Edema: whole body
Pulse rate : 82/min
Respiratory rate: 19/min
BP: 130/90mm/ Hg
SpO2: 97%
GRBS:231mg/dl
○SYSTEMIC EXAMINATION:
CVS:
Precordium is normal
Thrills absent
S1 and S2 heard.
No murmurs heard.
RS:
Chest is elliptical
Trachea: Central
Symmetrical expansion of chest.
Vesicular breath sounds heard.
No adventitious breath sounds heard.
ABDOMEN:
Abdomen is distended
Moves symmetrically with respiration
Umbulicus is central and inverted
No scars or sinuses
No local rise in temperature
No Tenderness .
CVS:
Precordium is normal
Thrills absent
S1 and S2 heard.
No murmurs heard.
RS:
Chest is elliptical
Trachea: Central
Symmetrical expansion of chest.
Vesicular breath sounds heard.
No adventitious breath sounds heard.
ABDOMEN:
Abdomen is distended
Moves symmetrically with respiration
Umbulicus is central and inverted
No scars or sinuses
No local rise in temperature
No Tenderness .
No palpable mass
No organomegally
CNS:
Higher mental functions normal.
Cerebellar functions normal.
Cranial nerve examination normal.
Sensory examination: decreased sensation of bilateral lower limbs.
No organomegally
CNS:
Higher mental functions normal.
Cerebellar functions normal.
Cranial nerve examination normal.
Sensory examination: decreased sensation of bilateral lower limbs.
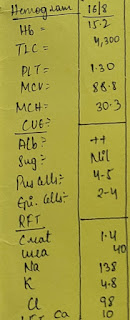
○Investigations :
●ECG
●Serum creatinine: 8.6mg/dl
●Blood urea: 124mg/dl
●RBS : 197mg/dl
●Complete urine examination :
Colour: pale yellow
Appearence: clear
Reaction: Acidic
Specific gravity : 1.010
Albumin : ++
Sugar : +
Bile salts: nil
Bile pigments: nil
Pus cells: 4-6
Epithelial cells: 2-4
RBC:nil
Crystals: nil
Cast: nil
Amorphous deposits: Absent
Others: nil
●Complete blood picture:
Blood group: AB
RH Typing : +
Haemoglobin : 6.8gm/dl
Total count : 10,900cells/cumm
Neutrophils: 86%
Lymphocytes : 06%
Eosinophils : 03%
Basophils : 00%
Monocytes : 05%
Platelet count :1.41 lakhs/cumm
Smear :
NORMOCYTIC NORMOCHROMIC Anemia with neutrophilic leucocytes and mild thrombocytopenia
●Liver function test :
Total bilirubin : 0.71mg/dl
Direct bilirubin : 0.20mg/dl
SGOT(AST) : 14IU/L
SGPT(ALT) : 09IU/L
Alkaline phosphate : 249IU/L
Total proteins : 6.0 gm/dl
Albumin : 2.91gm/dl
A/G Ratio : 0.94
●RFT
Urea : 122 mg/dl
Creatinine : 8.5 mg/dl
Uric acid : 8.8 mg/dl
Calcium : 8.8 mg/dl
Phosphorus : 6.4 mg/dl
Sodium : 139 mEq/L
Pottasium : 4.1 mEq/L
Chloride : 99 mEq/L
●Serum iron : 53ug/dl
●HBsAg-RAPID : Negative
● RTPCR for COVID-19 : POSITIVE
○Diagnosis :
Chronic renal failure
○Treatment:
▪︎Dialysis initiated on 11/2/2022
▪︎ Inj Lasix 40mg - PO / BD
Inj OROFER-XT - PO / OD
Inj NODOSIS 500 mg - PO / BD
Inj Sheileal - PO/OD
Tab met-xl 50mg -PO/OD
Tab Amlodipine 10mg -PO/OD
Tab LEVOGEN -PO/OD

Comments
Post a Comment